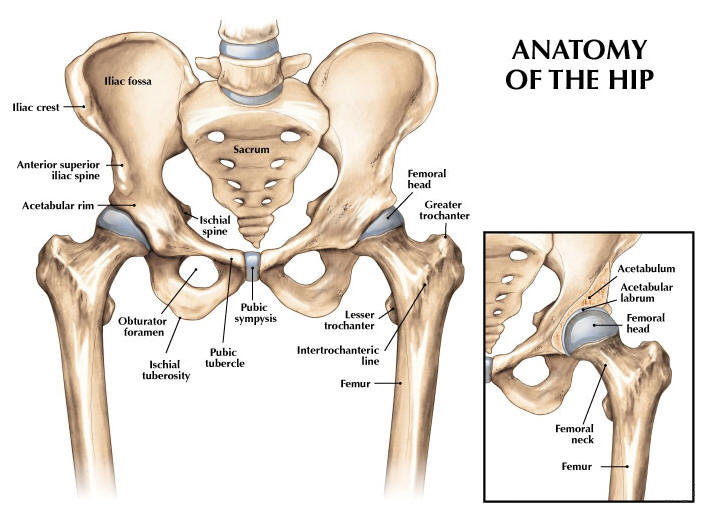
The hip joint is composed of two main bone parts: the Acetabulum and the Femur.
Acetabulum is the concave part of the pelvis where the femoral head is attached into.
Types of Fractures
Hip fractures are classified as either intracapsular or extracapsular fracture. By the word itself, intracapsular fractures occur at the part of the femur which is attached to the acetabulum. While extracapsular fractures are those found outside of that capsule and below.
To give you a more clear picture of the distinction, make an imaginary line from the tip of the greater trochanter to the tip of the lesser trochanter. The fractures that occur above of that line are your intracapsular fracture. And the one that occurs below are your extracapsular fractures.
Surgical Procedures
These are the common procedures that is done to fix a hip fracture.
Hip hemiarthroplasty is a surgical procedure done to fix an intracapsular fracture of the hip. It involves removing the femoral head and neck. Then, put a combination of prosthetics which includes a head, a neck, and a cemented stem.
Instruments and software that you may need during the procedure.
Trays.
Hip hemiarthroplasty tray
Stryker 6/7/8
Plug trials
Femoral rasps
Femoral basic instruments
Unipolar instruments
Softwares.
Hip pack
Crepe (optional)
Big ioban
Shark
Pulse lavage
1L PNSS
Saw blade (Please check surgeon’s preference; some likes wide blade, while others like the narrow one.)
Femoral brush (Mr OKB like femoral tip instead of the brush)
Suction catheter (f10 or f14)
Ribbon gauze
Optivac cement 80
1 vicryl (9465) x 2
2 polysorb
3 monocryl
Skin glue
Mepilex dressing
The procedure in a glance.
The procedure is done the following order (but may change as per circumstances or surgeon’s preference):
Skin preparation and draping.
Ground sheet.
U drape.
Foot drape.
Leggings.
Crepe (This is per surgeon’s preference. Some doesn’t use crepe.)
Hip drape.
Top drape.
Small ioban – may assist the surgeons by holding the leg.
Big ioban.
Set up your light handles, diathermy, suction, and pulse lavage.
Skin incision and fracture site preparation.
You may need the following instruments: scalpel, mayo scissors, norfolk and norwich, langenbecks, spikes, hohmann’s, charnley retractor, bristow.
Removal of the femur head.
Saw blade, nibbler, osteotome, mallet, cork screw, head measure, and have a skid handy.
Have a small ready for the acetabulum.
Some surgeons like to trial the head using unipolar trial heads on a handle.
Determine head size.
Femoral preparation.
Box chisel and mallet
Femoral reamers, starting from the smallest.
Plug sizer
Femoral rasps/sizer and handle; and have a t-handled charnley spoon ready.
Once they have determined the femoral stem size, they may trial it with a langenbeck and/or trial head.
When they are happy, they will install the cement plug and will prep the femur using the following: femoral brush (or tip for Mr OKB), suction catheter, and ribbon gauze (some surgeons will use the smallest plug sizer to introduce the ribbon gauze into the femoral cavity).
Cement and prosthesis.
Change gloves.
Always ask the surgeon if they’re happy for you to mix cement. It is also crucial to inform your runner and the anesthetic team that you will be cementing soon.
Mix the cement:
Mix for 30 seconds
Install nozzle and attach into the cement gun
Ideally, the surgeons will start introducing the cement 2 minutes after mixing.
Prosthesis:
Stem
Have the stem introducer ready (some surgeon would only use a mayo scissor to introduce the stem)
Gillies and mcdonald’s handy on the working table.
Ideally, will let the cement settle for 10 minutes.
Neck
Trial neck attached to a head trial.
Once they are happy, they will install the neck using the impactor and mallet.
Head
Impactor and mallet.
Skin closure.
1 vicryl x 2
2 vicryl
3 monocryl
skin glue
mepilex
Always make sure that you have checked the diathermy site and overall skin quality of the patient after the procedure; most important, sign out.